RNM-Care That’s Ethical, Advanced & Personalized
“We know these therapies don’t just prolong lives-they restore dignity, reduce suffering, and bring peace to families of cancer patients. That’s why we’re here.” We look forward to giving patients access to advanced, accessible and compassionate radionuclide therapies close to home in very personalized setting away from very busy corporate and government settings.

RNM is the first comprehensive dedicated nuclear medicine and theranostic center in Rohtak, Haryana to offer dedicated, advanced nuclear medicine services, including advanced precise- targeted radionuclide therapy for oncology and endocrine indications. Led by AIIMS and PGIMER-trained specialists, RNM emphasizes evidence-based protocols and compassionate care, providing accessible treatments away from crowded metropolitan hospitals.
To provide nuclear medicine facilities in the hinterlands, bringing world-class, ethical services to patients without the need to travel to metropolitan areas.
Highly qualified professional team of AIIMS and PGIMER trained doctors led by Dr. Parveen Kundu, MBBS (AIIMS), MD (Nuclear Medicine, AIIMS), FANMB with over 15 years of nuclear medicine and therapy experience.
A team of highly qualified professionals- physicists, technologist and nurses committed to delivering personalized radionuclide therapies.


with over 15 years of dedicated experience in radionuclide therapy.



An emerging radioligand treatment targeting cancer-associated fibroblasts (CAFs) prevalent in the tumor microenvironment of various solid tumors.
Indications:
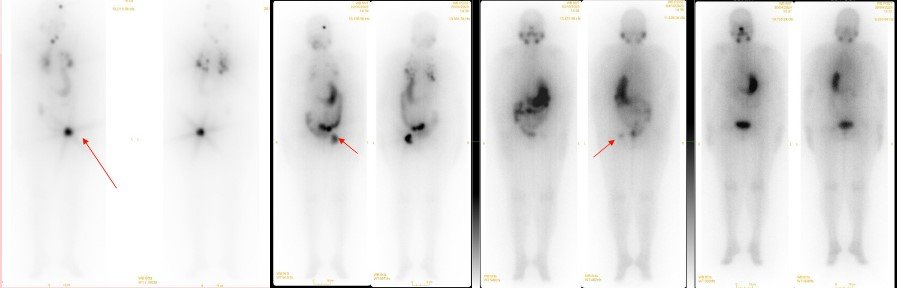
61y/ F total thyroidectomy and central neck dissection; post left femoral resection and endoprosthesis reconstruction on 01-07-22 HPE- residual follicular carcinoma in left lobe of thyroid, LN -ve; metastatic follicular carcinoma of thyroid

WhatsApp us
